










Should Canada’s younger veterans, including those who served in such hotspots as Bosnia, Rwanda, Cyprus and Afghanistan, be guaranteed priority access to long-term care beds? Some say it is the least we can do for those who put their lives on the line for Canada.
Dale Graham, a 73-year-old retired Canadian Armed Forces sergeant, is looking tired and worried on this late fall day at Dartmouth General Hospital in Nova Scotia.
Graham has prostate cancer. Decades ago, he was exposed to Agent Orange while serving at CFB Gagetown in New Brunswick. Exposure to the highly poisonous herbicide has been linked to increased risk of prostate cancer. He has received compensation for that exposure. Meanwhile, his cancer has spread, and led to other health problems. “You lose your balance…your nerves go all wacky.” He’d fallen about six weeks earlier, hurt a leg and lay helpless and cold for hours until a friend found him.
![Dale Graham awaits a long-term care bed to open up. [PHOTO: SHARON ADAMS]](https://legionmagazine.com/wp-content/uploads/2014/07/access1.jpg)
Unable to return home to live alone, Graham joined the wait list for long-term care and is fretting about how long it will be before a bed opens up. “The guy before me spent months in here,” he said.
Ironically, about 20 minutes away just across the harbour in Halifax, Camp Hill Veterans’ Memorial Building has no waiting list—but Graham, a “modern” veteran, does not qualify for long-term care there.
Camp Hill’s rooms are “contract beds”—spaces in provincial facilities to which “traditional” veterans have priority access under a funding agreement with Veterans Affairs Canada (VAC). “By legislation, contract beds are available to support eligible Second World War and Korean War veterans,” explained Janice Summerby, VAC spokesperson.
About 2,500 of the 8,500 veterans VAC supports in long-term care are traditional veterans in contract beds. But the contract arrangement and some dedicated veterans’ facilities will disappear with the traditional veterans (The Duty To Care, May/June 2014).
Despite efforts of veterans’ advocates, amendments have not been made to add modern veterans to legislation covering traditional veterans, nor has new legislation been passed granting modern veterans priority access to long-term care.
“I think it’s crap,” Graham said, citing dangerous deployments to Egypt, Cyprus and Congo during his 20 years of service ending in 1978. “You’re still carrying a gun.”
Veterans’ advocates agree. “Regardless of when and where a veteran served, the government has a duty of care,” said Gordon Moore, Dominion President of The Royal Canadian Legion. But there is disagreement about how far that duty should extend.
Although advocates are fond of saying “a veteran is a veteran is a veteran,” legislatively, this is not so. Over the years, 15 different eligibility classes have evolved for VAC long-term care, noted a 2013 report from Veterans Ombudsman Guy Parent. Modern veterans have the least access to long-term care benefits. Traditional veterans who served overseas have the broadest benefits, including priority access to long-term care as well as access to specialized veterans’ facilities and enriched programs.
Modern veterans who need long-term care for service-related disabilities will continue to be supported in provincial facilities by VAC. But before they apply for VAC support and benefits, they must meet provincial long-term care eligibility criteria which differ from province to province. Generally what’s required is proof of need of 24-hour care coupled with lack of support at home—and urgent cases take priority. There is no tick box for military service. Veterans like Graham queue up with civilians on provincial wait lists.
Having to join a wait list does not acknowledge the debt of gratitude owed to those who put their lives or health in jeopardy in service of their country; nor does it acknowledge that military service has the same effect on modern veterans as on Second World War and Korean War veterans, said Gordon Jenkins, president of the NATO Veterans Organization of Canada.
Military training, deployment and combat increase the risk of health problems which may develop years after service, or worsen with aging. These include arthritis, mental health issues, sickness from exposure to chemicals or exotic diseases, brain injury and hearing loss.
Modern and traditional veterans, regardless of where and when they served, have been exposed to such risks. All that sets the two groups apart is legislation, and legislation “can be changed at the stroke of a pen,” noted veterans advocate Sean Bruyea, a retired Canadian Armed Forces captain.
Amendments to the New Veterans Charter, now under review by the Commons Standing Committee on Veterans Affairs, could enrich modern veterans’ long-term care options. Veterans Affairs Minister Julian Fantino has requested the committee also include a definition of the social contract between veterans and the government.
“This is a key issue,” said veteran Duane Daly, a board member of the Perley and Rideau Veterans’ Health Centre in Ottawa and former Royal Canadian Legion dominion secretary. The federal government argues it should not be tied to commitments made by earlier governments dating back to the First World War. But “the commitment of unlimited liability of service that a veteran undertakes hasn’t changed since the First World War,” said Daly. Neither, he said, should the government’s responsibility for looking after veterans.
Having to join a wait list does not acknowledge the debt of gratitude owed to those who put their lives or health in jeopardy in service of their country.
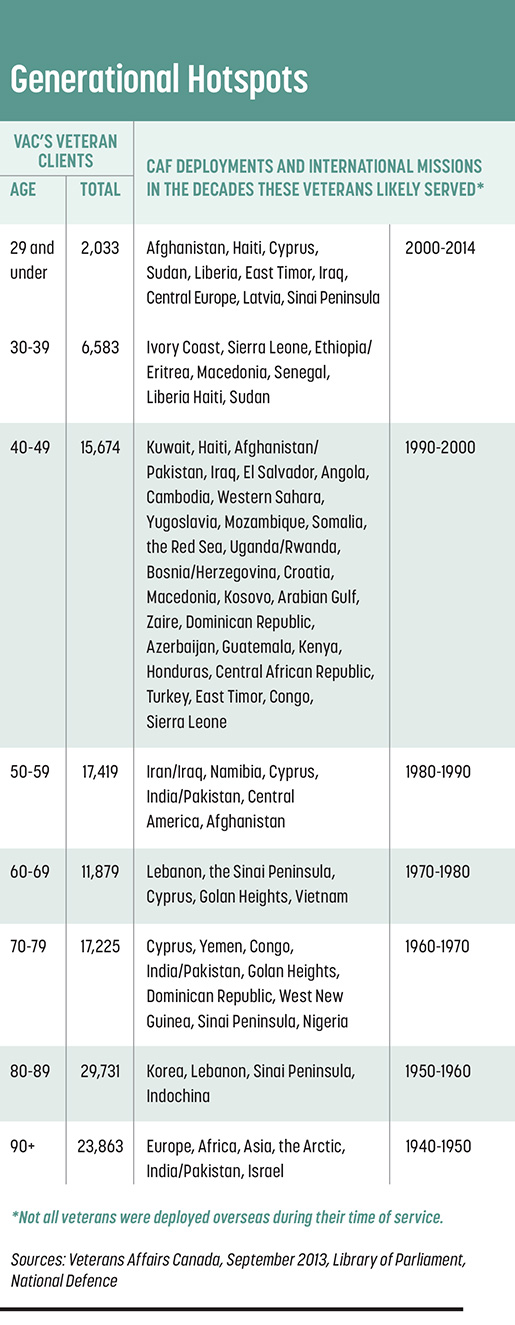
When provinces took over responsibility for health care decades ago, the idea for VAC to contract priority access beds “was a reasonable compromise to the closing down of veterans’ hospitals,” added Daly. But it is not reasonable to dismantle the system now as modern veterans enter the age when they might need long-term care. Veterans Affairs clients include nearly 19,000 modern veterans aged 70 to 79 and 15,000 aged 60 to 69.
Modern veterans will rely on provinces already having trouble coping with the overall long-term care demand. In Ontario, for example, the wait list increased between 2005 and 2012 by nearly 85 per cent while beds increased only three per cent, resulting in wait times of 94 days for clients in crisis and up to 14 months for moderate-need clients, noted the 2012 auditor general’s report.
Some provinces have plans for priority access beds. In a 2013 news report, Nova Scotia’s deputy minister of health and wellness described gradual release of the 334 beds reserved for veterans as “opportunities” to address the long-term care gap.
“We have to maintain the infrastructure of the contracted facilities so they can continue to serve modern veterans,” said Daly, with changes to reflect modern needs. “Once that infrastructure is gone, it will be impossible to rebuild.”
“Expansion of this benefit to all veterans would be a duplication of an existing provincial service,” said Summerby. Besides, modern veterans “are choosing to stay in long-term care facilities in their own communities…” Veterans Affairs Canada will pay the full cost of care of modern veterans with service-related injuries in provincial facilities close to their families; it now supports about 450.
But “simply paying the bills does not honour the covenant” between those who serve and the people of Canada, counters the Royal United Services Institute of Nova Scotia (RUSI). It recommends VAC institute similar contract arrangements for modern veterans as for traditional veterans, with modifications to accommodate needs of younger veterans.
In dedicated veterans’ facilities, staff are better acquainted with veterans’ unique health needs and staffing levels are better, said RUSI member Dr. Heather MacKinnon whose Halifax medical practice includes many veterans. Veterans’ homes like Camp Hill in Halifax are a focal point for VAC, veterans’ advocates, military organizations and community volunteers, ensuring veterans “are not fighting for every little thing they need.”
Veterans should have the added option of dedicated veterans’ homes with specialized programs that also keep them mentally alert and socially engaged, Daly argues.
Veteran Mike Sellar spent part of his nearly 12-year military career crawling into aircraft fuel tanks for inspection and maintenance, activities later linked to his diagnosis at age 29 with multiple sclerosis.
His symptoms gradually worsened after his release in 1991 until eventually he became bedridden. His wife Alisa looked after him for four years until his medical needs increased. After nine months on Nova Scotia’s wait list he was placed in a facility that is a 50-minute drive from home. Alisa was glad when he was transferred four months later to one of the residences at Parkland at the Lakes, in Dartmouth, a 20-minute drive from home.
Sellar’s room is bright and well-appointed, and VAC looks after his non-medical needs. Alisa visits nearly every day and military friends pop by, but there isn’t much to tempt him out of his room should he want some unscheduled company—he is much younger than most other residents, and the only veteran, in his building.
Sellar did not want to be placed in a veterans’ home, fearing he would not have much in common with much older veterans. But he does miss the company of those who’ve shared the culture. “They get you,” he said.
![Alisa Sellar visits her husband Mike almost daily in a long-term care facility in their community. [PHOTO: SHARON ADAMS]](https://legionmagazine.com/wp-content/uploads/2014/07/access2.jpg)
“It’s a tragedy all veterans aren’t able to get into (places) where they’ll feel more comfortable,” added Sellar’s friend and veterans’ advocate Roland Lawless. That is happening in some facilities with a history of serving veterans. At the Perley and Rideau Veterans’ Health Centre in Ottawa, a certain proportion of assisted-living apartments are reserved for veterans, said Akos Hoffer, chief executive officer.
Second World War veterans Bill Booth and Les Copan and modern veteran Hector Nicolson were drawn to Chelsea Park in Vancouver, one of 19 New Chelsea Society properties. A Legion initiative, the Society began providing affordable housing for veterans and their families in the 1950s, expanding over the years to meet community needs for affordable, supportive and seniors’ housing.
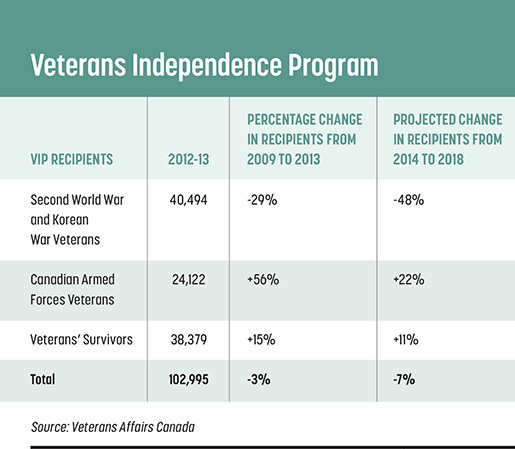
But there are other aspects to the long-term care picture. Advocates also want wider access for modern veterans to VAC’s Veterans Independence Program which provides services and support to help veterans age in their own homes. The Legion’s position is the government has a responsibility to ensure veterans with injuries attributable to their service have access to care and services that they need, explained Ray McInnis, director of the Legion’s Dominion Command Service Bureau in Ottawa. It is not necessary to replicate the benefits of the Pension Act for Second World War veterans, but the system does need to be modernized.
Modern veterans span all age groups, are spread across the country, have access to long-term care in their own communities and like most Canadians today, want to age at home as long as they can.
Institutional care is not the only answer, explained McInnis. The Legion wants the government to focus on the Veterans Independence Program so veterans and seniors can remain in their homes as long as possible.
The Legion and other veterans advocates want to see changes to the VIP, which now covers primarily housekeeping and yard work but “only if you fit the criteria,” said Ron Griffis, national president of the Canadian Association of Veterans in United Nations Peacekeeping. As with long-term care, modern veterans have the least access to VIP.
The Legion also believes that the complex eligibility criteria for veterans and spouses needs to be reduced, the application process simplified and programs and supports expanded.
“Now they’ll come around and clean your house or cut your grass, but there’s no provision for a handyman allowance if the doorknob falls off, or if your furnace is not working,” said Jenkins. “You could have a well-fed veteran living in a hovel.”
Veterans Ombudsman Guy Parent also suggests further study of assisted living options for veterans who need more support than VIP offers, but whose illnesses or disabilities are not severe enough to warrant long-term care. “Assisted living can bridge that gap,” says his 2014 review of the issue.
The issue of long-term care and support for veterans as they age deserves more public debate, said Daly, who fears “in 10 years time veterans in long-term care and needing specialized assistance” won’t know they could get help from VAC, and that a Legion service officer will help press their cases.
Over time, Daly fears, veterans and society at large will forget the full responsibility the federal government has to care for veterans.
Advertisement







