



![. [ILLUSTRATION: STEPHEN SNIDER]](https://legionmagazine.com/wp-content/uploads/2008/10/vipleadnd.jpg)
Second World War veteran Phil Bradbury, 85, of Toronto was surprised to learn that in civilian life he’d been missing in action for a couple of decades. Veterans Affairs Canada has been looking for veterans like Bradbury who qualify for, but aren’t receiving benefits under the Veterans Independence Program. The VIP helps aging veterans live independently as long as possible by providing home care support like housecleaning and shovelling walkways, making meals and help with bathing, as well as home adaptation and health support services.
Bradbury was on the crew of a bomber that flew 34 missions near the end of the Second World War. All seven crew members survived the war, but not unscathed. “I was injured a number of times.” Five of their planes were destroyed and barely made it back to base. Twice they crash-landed and the whole crew was put on medical leave. Bradbury suffered head and back injuries and was once pulled unconscious from a burning aircraft. His injuries caused him to black out at work at first after he’d resumed civilian life, and have magnified the health conditions that typically plague people in their sunset years.
![Phil Bradbury survived 34 bomber missions during the Second World War. War injuries magnify the health problems of aging. [PHOTO: PHIL BRADBURY]](https://legionmagazine.com/wp-content/uploads/2008/10/vipspot1nd.jpg)
He’s been receiving a VAC pension for service-related hearing loss and other injuries for better than five decades. He retired in the late 1980s. “Financially I’d never suffered. If I had, perhaps I would have pursued it.”
It was a financial pinch that resulted in his discovering the VIP program. His doctor switched him from one heart medication, which caused side effects, to a more expensive drug, one the Ontario Health Insurance Plan does not cover. Bradbury complained about it to his brother-in-law, a veteran of the Korean War, who is on VIP, and who told him about the program’s benefits.
Bradbury applied right away. A case manager visited him and his wife Bernice about a year ago to determine his eligibility for VIP and other services. Veterans Affairs started picking up the medication tab right away and he learned he was eligible for more support, like a walker and chiropractic care. He was advised about VIP benefits, including those that would carry on for Bernice. “I think it’s just great,” says Bradbury.
![. [.]](https://legionmagazine.com/wp-content/uploads/2008/10/vipblurb1.jpg)
Although the program goes some way in paying our national debt of gratitude to veterans and their families, it’s not sentiment but economics that’s driving Veterans Affairs Canada to try to reach qualifying veterans and their caregivers not taking advantage of the program. With some help, many can live independently in their own homes, putting off, maybe even avoiding, the day they go into long-term care. Fewer health care dollars are spent supporting them at home than in supplying those same services in a facility, and fewer facilities need to be built and maintained.
“At Sunnybrook Hospital, it costs about $100,000 per bed annually to keep a veteran in the hospital,” Veterans Affairs Minister Greg Thompson told the House of Commons Standing Committee on Veterans Affairs at a hearing in March. “The fact is this veteran could have stayed at home at a much cheaper cost to the Government of Canada and enjoyed those few years at home as opposed to going into a facility.”
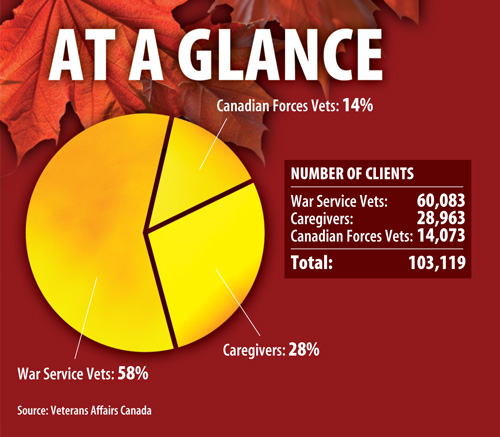
There are 103,119 war service veterans, Canadian Forces veterans and caregivers currently receiving VIP benefits, but there are probably tens of thousands more who qualify for benefits, estimates Rob Anders, chairman of the Standing Committee on Veterans Affairs. “We recognize we are dealing with a generation of people…who believe if they can help themselves, that’s the way it should be,” says Anders. “But we also don’t want to have these people suffer unduly for that (or) wind up putting themselves in a full-care facility before they really need to.”
The VIP program has been such a success, The Royal Canadian Legion is advocating not only for VIP to be extended to all of Canada’s approximate 600,000 veterans who need its help, but to all Canadian seniors in need through a national Seniors Independence Program. And some provinces are using the program as a template for restructuring their own health care programs to develop more economic long-term care in anticipation of the baby boomer bulge moving through their systems.
“We have evidence…costs are typically 40 to 70 per cent lower,” so long as the home care services are substituted for similar services in a long-term care facility, says health economist Marcus Hollander, president of Hollander Analytical Services, a Victoria-based health research firm.
![Lorraine Chace with a portrait of Bill, her husband of 50 years. Bill died before applying for the full menu of VIP benefits, and she can’t apply for them herself. [PHOTO: SHARON ADAMS]](https://legionmagazine.com/wp-content/uploads/2008/10/vipspot3nd.jpg)
Some of that evidence comes from a real-world ‘natural experiment’ in British Columbia that show the cost savings for home care programs like VIP. In the mid-1980s home care services were substituted for institutional care. A decade later, 9,993 fewer long-term care beds were in use—at an annual savings of about $150 million in British Columbia, Hollander says. One big reason for the savings is that “90 per cent of services delivered” in a facility are supportive, rather than professional care. He found average annual costs to government for people with moderate care needs was $9,624 for home care and $25,742 in institutions. At the highest level of care, corresponding costs were $34,859 for home care and $44,233 for institution care.
British Columbia also discovered what happens to health care costs when even basic home care services are discontinued when in the mid-1990s some financially strapped health care regions cut housecleaning services while others did not. After three years, it was discovered that each client cut from this lowest level of service cost the health care system $3,200 more in annual acute and long-term care costs.
Take away supportive services, says Hollander, health deteriorates more quickly, and seniors go into a long-term care facility sooner. “Very modest investments in home care can have big results in the longer term,” he says. But “the crux is policy-makers don’t understand this.” Instead, care and budgets are fragmented, home care often coming from a social services budget. Even when considered part of the continuum of long-term care, supportive home care services are often sacrificed during cost-savings.
But policy-makers can be educated. When shown that about $30 million could be shaved annually by shifting services for 1,121 seniors from long-term care to home services, “our government really did sit up and take notice,” says Kathy Greenwood, director of services and business support for the continuing care branch of the Nova Scotia Department of Health.
It resulted in support for a 10-year strategic plan, now in year three, to build a sustainable system that includes home care as part of the continuum of services. “We’ve spent a fair bit of time talking to Veterans Affairs about their success (with VIP).” Although the province currently has a home care program for its own citizens with services on a sliding scale based on income, it does not yet include some of the features of VIP. One example, she said, is grounds maintenance, a key service to helping seniors stay in their own homes when they can no longer mow the lawn or shovel snow.
So if home care programs save money in the long term, why isn’t VIP available to every veteran who needs it? Simply put, policy-makers have to balance long-term savings against the depth of their pockets at the moment. “You have to invest in it,” says Darragh Mogan, director general program and service policy division, veterans’ services, in Charlottetown. And “governments have to weigh other investments they might want to make in roads and schools and economic development; it’s in the balance of considerations.”
“There are many other groups and needs out there,” adds Anders. “Rest assured we are putting more into this and it’s just a question of shuffling resources between various needs.” The Veterans Affairs budget is $545 million more than what it was in 2005-06, bringing it to approximately $3.4 billion.
But politicians also worry about “picking up more people and therefore increasing overall costs,” explains Mogan.
![. [.]](https://legionmagazine.com/wp-content/uploads/2008/10/vipblurb2.jpg)
But Veterans Affairs overestimates the cost of program expansion, says Pierre Allard, Director of The Royal Canadian Legion’s Service Bureau at Dominion Command, which helps veterans apply for VIP and disability benefits. He gives the example of an expansion in 2003 of benefits for widows, who had been covered for only one year following the death of their veteran husband. VAC estimated it would cost $243 million to extend VIP housekeeping and grounds maintenance benefits to surviving primary caregivers back to 1981 and increase them from a one-year to a lifetime benefit. As of March 31, 2008, $72 million had been spent on reinstatements and $80.5 million on lifetime continuations. “We see a trend where the government consistently overestimates the cost of improvements to VIP,” adds Allard.
“They try to determine all the eligible people that will come forward, while in effect, only a percentage of all eligible people come forward,” he says. VAC says about 21,900 survivors were expected to apply for reinstatements, but 12,400 came forward in 2005-06—about 57 per cent of those eligible, but the department continues to try to enlist more.
Those that do come forward don’t always take all the benefits to which they’re entitled, says Allard. That was a common comment from VIP recipients interviewed for this story.
Although VAC offered nursing and other benefits to William and Clare Kobes in Calgary, they turned them down. “I was able to look after him,” says Clare. “We had saved money and we really felt there were other people who needed it more.”
![Mary Monteith relies on VIP’s housekeeping and groundskeeping services for chores she no longer can handle since being injured in a training exercise. [PHOTO: SHARON ADAMS]](https://legionmagazine.com/wp-content/uploads/2008/10/vipspot2nd.jpg)
“I don’t claim for a lot of things I could claim for because I’m sort of financially fit,” says Bradbury. “I’m not wealthy, but I can get by.”
Some VIP recipients don’t take the maximum allowed for one service. “They wanted to send somebody four times a week,” for housecleaning, adds George Henderson Armet of Montreal, “but once a week is good enough.” Still others wait until their need is great before taking a benefit. VIP has offered Bradbury a chair that tilts to help him stand but he thinks he doesn’t need it yet.
In choosing among spending options, the Legion urges politicians not to forget our obligation to veterans and their families. “We should not forget all the promises we made to veterans to look after them and their families if they did not come back or could not look after them,” says Allard. “It’s a simple element of trust.”
“Given recent research findings that stressful deployments can have latent long-term effects on health, it is particularly important for Canada to keep its promise to provide care for veterans,” says the Gerontological Advisory Council (GAC) in its 2006 report Keeping the Promise: The Future of Health Benefits for Canada’s War Veterans. It suggests combining VAC health and social programs to create Veterans Integrated Services, a needs-based continuum of care that would do away with many of the complaints about VIP and other VAC programs.
![. [.]](https://legionmagazine.com/wp-content/uploads/2008/10/vipblurb3.jpg)
The biggest complaints about VIP are ineligibility and complexity of the eligibility and application processes. The Legion and others advocate extending VIP to all frail veterans, to Allied veterans, widows and caregivers and RCMP members and veterans. “All widows should receive VIP, regardless of what their income is,” says Joyce Carter, 81, of Cape Breton. “They all struggled to look after their husbands for years after they came out of the forces. If they weren’t wounded, they certainly were traumatized by what they saw.”
Lack of funds is no excuse, adds Carter, a tireless campaigner for widows’ rights to VIP. “The government finds money for issues that are less important, and they do it without any debate or review.” When Carter’s husband Murdock died in 2000, after 55 years of marriage, rules at the time allowed veterans’ survivors to continue collecting benefits for one year. When cut off, many were left in desperate straits.
“I was devastated,” she says. “You feel destitute.” So she began a campaign to have benefits for widows of qualifying veterans continue for life, a change made in 2003. She continues to lobby for widows’ benefits.
Michael Hill of Orangeville, Ont., is lobbying on behalf of Allied war veterans in Canada who lost VIP eligibility in 1995. “It’s a matter of principle,” he says. “They fought the fight on the right side. It’s a really big thing for those guys trying to stay in their own home.” And for the government “really, it’s chump change. It’s a sunset clause, because they’re dying off rapidly. It’s the worst injustice trying to save a couple of dollars with people we owe so much to.”
Allied veteran Bill Edge, 85, is offended his benefits were cut off. “Really, I feel like a second-class citizen in a first-class country.”
![Allied veteran Bill Edge fought under the same flag as Canadians, but despite living in Canada for more than 50 years, is not eligible for VIP services. [PHOTO: ORANGEVILLE BANNER]](https://legionmagazine.com/wp-content/uploads/2008/10/vipspot4nd.jpg)
He served in the Royal Corps of Signals during the Second World War and moved to Canada in the early 1950s. When he retired in 1988 he was given a card saying he was a member of the VIP program. “I never had a chance to even use it” before Allied veterans lost entitlement in 1995. What stings is “I’d been sent a letter saying I’d been grandfathered in. I’ve been in Canada 66 years. I was on the beaches on D-Day; I fought through France and into Germany. I even fought for the Canadian forces” as part of an international army, led by a Canadian general and made up of one division of Polish troops and two divisions each of British, Canadian and American soldiers. “We fought under the same flag.”
His income totals about $2,200 a month, and he pays nearly a tenth of that on prostate cancer medicine not covered by OHIP. It’s getting harder to stay in his home. “I’m going to die here—or die in the attempt,” he says.
Flattening eligibility criteria would ensure all frail veterans have access to VIP benefits, as well as other services as needed. “One of the key gaps is that treatment benefits and VIP are available to only a small proportion of veterans,” says the GAC report. It estimates 70,000 veterans don’t qualify or aren’t receiving VIP or treatment benefits.
Frail veterans, few of whom can fight on their own for benefits, are of special concern to the Legion, says Allard. “The crux of the problem is that access mainly goes through being eligible for disability benefits.” But many veterans do not have a pensionable condition related to their war service, even though they have a number of health conditions that combine to make them frail. As well, perhaps 40 per cent of them suffer dementia.
Even Thompson, in his evidence before the Senate Subcommittee on Veterans Affairs in March, said it makes no sense that “some veterans, because they do not have a pensionable condition, are not eligible for the most low-cost and effective program we have, which is VIP,” but do qualify for more expensive long-term care.
“We have actually changed some… internal rules to extend VIP to some of these veterans who normally did not qualify and are in their frail stages of life,” Thompson told the committee.
![. [.]](https://legionmagazine.com/wp-content/uploads/2008/10/vipblurb4.jpg)
There are several ways for otherwise ineligible frail veterans to get VIP benefits, says Mogan. One is a program which offers home care to Second World War and Korean War veterans with nursing care needs waiting at home for a long-term bed. “We saw a need coming for about 20,000 additional long-term care beds.” In 1999, VIP benefits were offered to some of those waiting at home for long-term care. When the beds came open “95 per cent said they’d prefer to stay at home,” with home care support. The program was rolled out formally in 2003.
For frail veterans not eligible for VIP, or on a waiting list, “if a veteran is awarded a civil (disability) tax credit and is also frail, the two of them together would satisfy requirements for VIP,” says Mogan. Revenue Canada criteria cover blindness, life-sustaining therapy, an impairment for more than a year that prevents speaking, hearing or walking, independently using the toilet, feeding or dressing oneself, or performing mental functions necessary for everyday life. “We know in the population over 80, 10 to 15 per cent will suffer some sort of frailty as defined by Revenue Canada for a disability tax credit, and we use that criteria with some modifications,” says Mogan.
“It’s not 100 per cent—I don’t want to mislead you,” says Mogan, adding “we use a generous interpretation of existing authority” to include as many frail veterans as possible.
That may be practice, says Allard, but “it’s not policy.” Not everyone can know about it, and that leads to a lack of standardization, which can lead to one of the “horror stories” Allard and Legion service bureau officers deal with, where benefits are granted then after a period of time, reviewed and rescinded. “There’s a problem if it’s not written down.”
And there are still veterans in need who will not qualify. One veteran denied VIP “was 89, and his wife of 60 years went into chronic care,” says Quebec Command Service Officer Debra Viskelis. “He asked for basic housekeeping and was turned down.” His health did break down, after which the provincial health care system deemed him as needing chronic care. He then won his appeal for VIP because he now has multiple frailties. Would his health have held up if he’d been granted VIP earlier? “Who can say?” says Viskelis. “But housekeeping and groundskeeping is not even $3,000 per year; chronic care is going to cost them thousands a month potentially.”
Eligibility criteria and the application process for VIP, long-term care and treatment benefits are “very, very complex,” explains Allard. Part of the reason for that, he says, is that programs have evolved over time, and VAC “has tried to be more generous” by introducing more benefits and more categories so more applicants would qualify.
The GAC’s recommendation for integrated services would simplify eligibility and application processes by using one entry point, and result in a needs-based continuum of care with someone assigned to shepherd claimants through the system.
“In my view, VIP is an excellent program,” says Hollander. It’s “probably the only home care program that still has a clear maintenance and preventive function.” However, “to fully realize its potential, I think it needs to be incorporated into a broader, more integrated system of care” enabling “the kinds of trade-offs that allow you to provide good care and to save money.”
Such changes will enhance what is already a very successful program. “By and large the VIP program does operate smoothly,” says Allard.
Every veteran receiving VIP interviewed for this story was grateful for the benefits received. Many said without benefits, they would face financial hardship.
![. [.]](https://legionmagazine.com/wp-content/uploads/2008/10/vipblurb5.jpg)
For those on scarce income, paying for a service then waiting months for reimbursement is a hardship. Carter says she knows widows on poverty-level incomes waiting for reimbursement who have stopped housekeeping services because they can’t afford to continue paying for the service without regular reimbursement. “None of them can make ends meet,” she says. “It’s an awful struggle.”
Some complained about complex application procedures. “It’s complicated even for me,” says an adult son who fills out forms for his blind father, who must get copies of appointment slips and doctors’ signatures in order to file for reimbursement. His dad pays $300 a month for housekeeping and personal care and gets $1,400 a year for taxis to take him to social events. Since there’s a ceiling on payments, “the government should be more trusting with veterans; they’re not out to screw the system.”
“It sometimes seems to me it’s the accountants that are in charge of this program,” says Viskelis.
Some said more sensitivity is needed in dealing with aged veterans. “You’re treated like a number. Or a beggar,” says one 86-year-old veteran. Still, the veteran says, that could be the price of fairness, for VAC wants to make sure it is the veteran who is receiving the benefits, and that the veteran is not a victim of elder abuse.
Several said better communications would help. “All the veterans should be notified, each and every one, about what they’re entitled to,” says one Montreal veteran. Although qualifications for entitlement and changes to programs are published on the VAC website and in Salute, VAC’s quarterly, bilingual newspaper, the target clientele may not get or read the newsletter, says Viskelis. Allard notes a lack of advertisement of benefits in mass media. The standing committee report advises VAC to pay more attention to reaching rural and Aboriginal veterans, and suggests the department take advantage of the Legion’s nearly 1,500 branches spread across the country as a way to communicate with far-flung veterans.
The Legion is glad to help, says Allard, at all levels—from helping veterans apply for programs, and helping VAC shape programs to better suit the clientele. Veterans don’t need to be Legion members to ask for help, and help is available by contacting any of the Legion’s branches.
“VIP is a great program,” adds Allard. “It allows people to stay in their home, which is what they want to do. It gives them a level of comfort as they age. There are some elements of VIP that need to be looked at and copied across the country,” he says, even if Canada’s fragmented approach to health care would make a national seniors independence program a challenge. “Is there a simple solution?” he asks. “Probably not; but it is a very, very good program, which is why we’d like to see it across Canada.”
Click to view VIP At A Glance.
Email the writer at: writer@legionmagazine.com
Email a letter to the editor at: letters@legionmagazine.com
Advertisement

